Menopause weight management: why your body is changing and what actually works

If you have noticed the scale creeping up despite eating the same way you always have, you are not imagining things. Menopause weight management is one of the most searched — and most misunderstood — topics in women's health. You did not suddenly lose willpower. Your hormones shifted, and your body responded exactly as biology predicted it would.
This article covers the real reasons behind midlife weight gain, what the research actually says about diet and exercise at this stage, and which medical options are now available. I am Dr. Laura Hendricks, a Registered Dietitian Nutritionist and Certified Menopause Practitioner with 12 years of clinical experience working with perimenopausal and postmenopausal women. Everything here draws on peer-reviewed research, clinical guidelines from organizations including the North American Menopause Society (NAMS) and the British Menopause Society, and direct experience from my practice.
What is menopause weight management and why does it feel different this time?
You have probably tried cutting back on food before. It worked — at least somewhat. But now nothing seems to move the needle. That experience is not unusual. Menopause weight management is genuinely different from weight management at 30, and the reason is biology, not behavior.

Menopause is defined as 12 consecutive months without a menstrual period. It is typically preceded by several years of perimenopause — a phase marked by irregular periods and fluctuating hormone levels. After menopause, the postmenopause phase begins and hormone levels stabilize at a new, lower baseline.
According to research published in peer-reviewed literature and cited by the British Menopause Society, women gain an average of 1.5 kg (approximately 3.3 pounds) per year during perimenopause. Some studies estimate a total gain of 5–10 kg by the time full menopause is reached, depending on the individual.
But here is what matters more than the total number on the scale: where the weight goes.
The difference between perimenopause, menopause, and postmenopause weight gain
Many women come to me frustrated because they feel like their body changed overnight. In reality, the process often begins years before the final menstrual period.
During perimenopause, estrogen levels fluctuate unpredictably. This disrupts sleep, mood, appetite signals, and fat storage patterns simultaneously. Weight gain during this phase can feel sudden because several mechanisms activate at once.
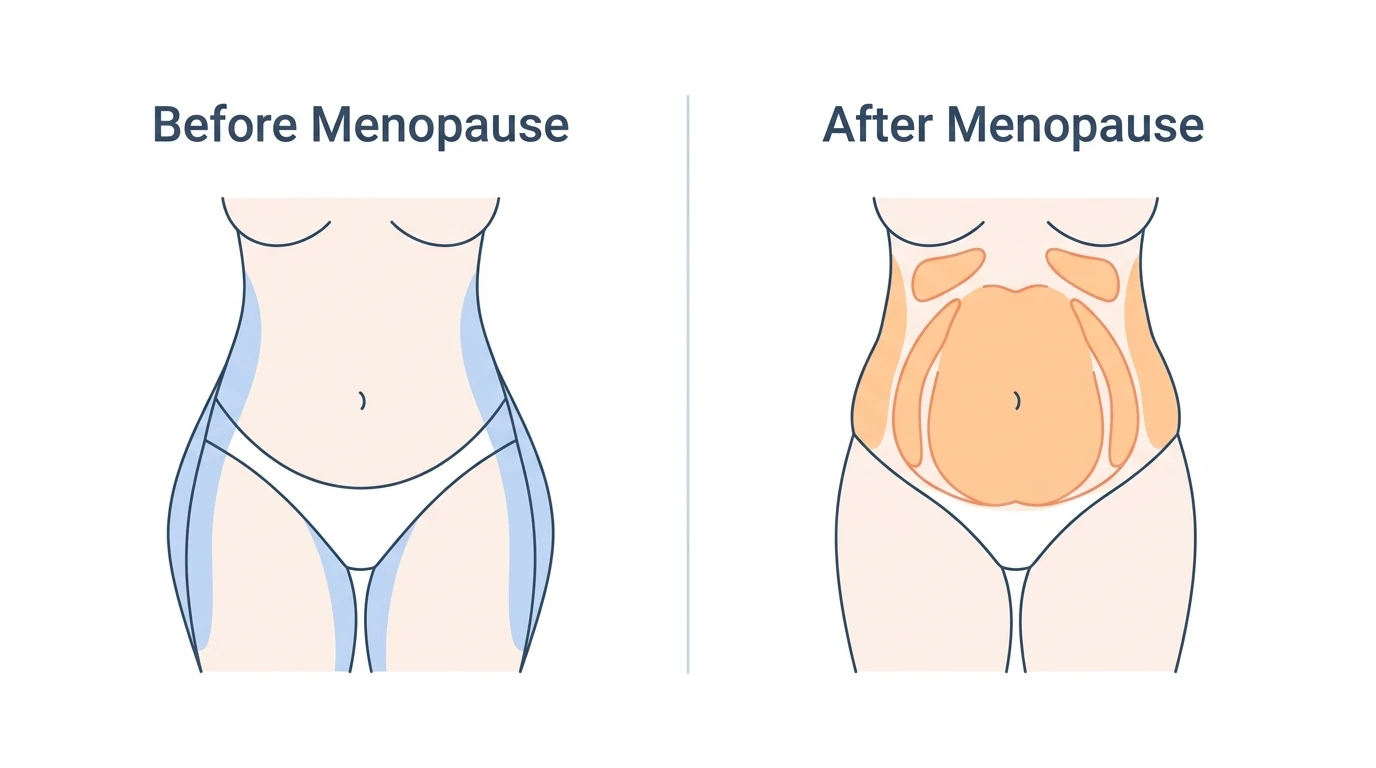
By full menopause, estrogen has declined significantly. The hormonal environment now favors storing fat in the abdomen rather than the hips and thighs. During postmenopause, this pattern typically continues unless addressed with targeted nutrition, exercise, and sometimes medical support.
If you are still getting a period but noticing changes in your weight and body shape, this article applies to you too. The weight challenges of menopause do not wait for the official 12-month mark.
Why belly fat specifically becomes the problem after menopause
This is the question I hear most often in my practice: "I've always carried weight on my hips. Why is it all going to my stomach now?"
The answer comes down to estrogen and weight gain. Estrogen plays a direct role in regulating where the body stores fat. When estrogen levels fall, the body shifts from storing fat subcutaneously — just under the skin on the hips, thighs, and buttocks — to storing it viscerally, deep inside the abdomen around the organs.
This distinction matters enormously for health. Visceral fat, sometimes called menopause belly fat, is metabolically active in a damaging way. It drives chronic inflammation, raises LDL cholesterol, impairs insulin sensitivity, and significantly increases the risk of cardiovascular disease, type 2 diabetes, and metabolic syndrome.
A 2022 review published in Metabolism: Clinical and Experimental confirmed that menopausal status and declining estrogen are independently associated with increased visceral fat accumulation, even after controlling for age and total body weight.
This is why menopause weight management is a health priority — not a vanity issue.
The real reasons behind menopause weight gain
Understanding why this is happening is the first step toward doing something effective about it. Most women have been told "eat less, move more." That advice is incomplete at best and counterproductive at worst when hormones, metabolism, and body composition are all shifting simultaneously.
Here are the four core drivers.

How declining estrogen changes the way your body stores fat
Estrogen does far more than regulate the menstrual cycle. It influences insulin sensitivity, fat distribution, physical activity drive, and appetite signaling through hormones like leptin and ghrelin.
When estrogen declines during the menopausal transition, several things happen at once. Insulin sensitivity decreases, meaning the body has to produce more insulin to manage blood sugar — and higher insulin levels promote fat storage. Appetite regulation becomes less stable. And fat storage shifts centrally, as described above.
Research shows that estrogen therapy can partly reverse this shift. A 2023 Mayo Clinic clinical review noted that menopausal hormone therapy can reduce visceral fat, improve insulin sensitivity, and lower the progression to type 2 diabetes in appropriately selected women. However, major guidelines including NAMS are clear: hormone therapy should not be prescribed purely for weight loss. Its primary role remains symptom relief and bone protection.
Progesterone and androgens also change during this transition. These shifts interact with sleep quality and appetite hormones, compounding the effect of estrogen decline — but estrogen remains the dominant factor in fat redistribution.
Aging, muscle loss, and a slower metabolism
Here is a question worth sitting with: How much of this is menopause, and how much is simply getting older?
The honest answer is both — and they work together.
From approximately age 30 onward, the body gradually loses lean muscle mass in a process called sarcopenia. Muscle tissue burns more calories at rest than fat tissue does. As muscle declines, resting energy expenditure — the calories your body burns just to keep you alive — drops accordingly.
A Mayo Clinic analysis found that age-related changes in body composition begin earlier than most women expect, often accelerating through the 40s well before perimenopause is recognized. By midlife, a woman's resting metabolism may be burning meaningfully fewer calories per day than it did in her 30s, even if her diet and exercise habits appear unchanged.
The math is straightforward and important: a daily caloric surplus of just 50–100 calories — less than a small handful of crackers — can result in several kilograms of weight gain over a decade. The body does not need a dramatic change to accumulate weight slowly.
This is not a reason for despair. It is a reason to target muscle preservation specifically — which is why strength training becomes the most important form of exercise at this stage of life.
The sleep and stress connection most women overlook
Poor sleep and elevated stress are not just uncomfortable side effects of menopause. They are direct drivers of menopause weight gain — and most general-audience articles underexplain this link.
Hot flashes and night sweats disrupt sleep architecture even when a woman does not fully wake up. Fragmented sleep raises cortisol, the primary stress hormone, and disrupts the balance between leptin (the hormone that signals fullness) and ghrelin (the hormone that signals hunger). The result is increased appetite the following day, with a particular drive toward high-sugar, high-calorie foods.
A large epidemiologic review cited by the British Menopause Society linked short sleep duration to significantly higher obesity and cardiometabolic risk — independent of diet and exercise habits.
Cortisol and menopause weight are also deeply connected. Chronic stress — whether from work demands, caregiving responsibilities, or the emotional weight of life transitions that often coincide with this stage — keeps cortisol elevated. Chronically high cortisol promotes abdominal fat storage specifically.
Mood changes including anxiety, low mood, and irritability are common during the menopausal transition. These changes can increase comfort eating and alcohol use. Both raise caloric intake and contribute to visceral fat accumulation when persistent.
None of this represents a failure of character. These are physiological processes responding to a genuine hormonal environment.
The gut microbiome's emerging role in menopause weight
This section sits at the frontier of current research, and it is worth including because it changes how we think about menopause metabolism changes.
Newer studies published in peer-reviewed journals including Metabolism: Clinical and Experimental show that the hormonal changes of menopause alter the diversity and composition of the gut microbiome — the trillions of bacteria that live in the digestive tract and influence almost every aspect of metabolic health.
These microbiome shifts change how the body responds to food. Post-meal blood sugar spikes become more pronounced. Blood fat responses become less favorable. And when the microbiome is dysregulated, visceral fat accumulation is more likely.
Circadian disruption compounds this effect. Late-night eating and irregular sleep-wake cycles further impair metabolic flexibility — the body's ability to switch between burning fat and burning sugar for energy — making weight loss harder and fat storage more likely.
Emerging programs, including gut microbiome-guided approaches, aim to personalize nutrition based on individual metabolic responses. While commercial offerings in this space vary significantly in quality, the underlying science is sound and growing. At MenoVitality, this evolving evidence informs how we think about gut health as part of comprehensive menopause support.
The best diet for menopause weight management
There is no shortage of dietary advice for menopausal women. The problem is that most of it is either too generic to be useful or too extreme to be sustainable. What follows is grounded in clinical guidelines and what I have seen work in practice over 12 years.

Why crash dieting makes menopause weight worse
Before addressing what to eat, it is worth addressing the most common mistake: severe caloric restriction.
Crash dieting lowers your resting metabolic rate. At a stage of life when your metabolism is already under pressure from muscle loss and hormonal changes, dramatically cutting calories signals to the body that food is scarce. The body responds by becoming more efficient — which means burning fewer calories, not fewer fat stores.
ZOE's research team, in a large cohort analysis, found that repeated cycles of restrictive dieting were associated with worsened metabolic outcomes in midlife women compared to those who maintained a consistent, moderate dietary approach.
The evidence-based target, supported by NAMS and the British Menopause Society, is a daily caloric deficit of approximately 500 calories — achieved through sustainable changes to eating patterns combined with regular exercise. This produces a weight loss of roughly 0.5 kg per week without triggering the metabolic downregulation associated with more extreme restriction.
Protein — the most important macronutrient during menopause
If there is one dietary change with the strongest evidence for menopausal women, it is increasing protein intake.
Protein preserves lean muscle mass during weight loss. It increases satiety, meaning you feel full for longer after eating. And it has a higher thermic effect than carbohydrates or fat — meaning the body burns more calories simply digesting it.
The clinical target most commonly cited in menopause-specific nutrition guidelines is approximately 1.2 grams of protein per kilogram of body weight per day. For a woman weighing 70 kg, that means roughly 84 grams of protein daily.
Practically, this translates to aiming for 20–40 grams of protein per meal. Good sources include eggs, Greek yogurt, cottage cheese, legumes, fish, chicken, tofu, and tempeh.
NAMS's practice pearl on dietary strategies for weight loss specifically highlights protein as essential for preserving body composition during caloric restriction in perimenopausal and postmenopausal women.
Fiber, plant diversity, and blood sugar stability
The second most important dietary target is fiber — specifically 25–30 grams per day, which most Western diets fall well short of.
Dietary fiber stabilizes blood sugar by slowing glucose absorption. It feeds beneficial gut bacteria, which supports the microbiome health discussed earlier. It increases satiety. And higher-fiber diets are consistently associated with lower visceral fat in population studies.
The foods that deliver the most fiber also happen to support the gut microbiome and reduce chronic inflammation: vegetables, fruits, whole grains, legumes, nuts, and seeds. This combination forms the backbone of the Mediterranean diet — the most extensively researched dietary pattern for menopausal women, with consistent evidence for improved cardiometabolic outcomes, lower visceral fat, and better weight maintenance compared to low-fat diets.
Plant diversity matters as much as total fiber intake. Research suggests that consuming 30 or more different plant foods per week — including herbs and spices — is associated with significantly greater gut microbiome diversity and lower metabolic disease risk.
What to reduce or eliminate for faster results
Knowing what to add is important. Knowing what to reduce is equally important — and often more actionable.
Three categories of food consistently appear in the evidence as drivers of menopause belly fat and metabolic dysfunction in midlife women.
Ultra-processed foods are the first target. These products — packaged snacks, fast food, sweetened breakfast cereals, processed deli meats — are engineered to be easy to overeat. They are calorie-dense, low in protein and fiber, and designed to bypass normal satiety signals. A 2019 randomized controlled trial published in Cell Metabolism found that participants eating an ultra-processed diet consumed an average of 500 more calories per day than those eating whole foods — without feeling any more hungry.
Refined sugars and liquid calories are the second target. Sugary drinks, fruit juices, flavored coffees, and alcohol spike blood sugar rapidly, promote insulin release, and contribute directly to visceral fat accumulation. They also deliver calories without triggering meaningful fullness.
Alcohol deserves specific mention. Beyond its caloric content, alcohol disrupts sleep quality — directly worsening the sleep-weight cycle described earlier — and increases the frequency and severity of hot flashes in many women. Research cited by the British Menopause Society links regular alcohol consumption to increased abdominal fat and elevated cardiometabolic risk in postmenopausal women.
The goal here is not elimination for its own sake. It is targeted reduction of the specific inputs that work against your hormonal environment at this stage of life.
Exercise that actually works for menopause weight management
Exercise advice for menopausal women is often frustratingly vague. "Move more." "Get your heart rate up." "Try yoga." These suggestions are not wrong, but they are incomplete. The type of exercise matters enormously at this stage — and most women are doing too much of the wrong kind and not enough of the right kind.
Why strength training is the priority, not cardio
One of the most common patterns I see in my practice: a woman starts gaining weight during perimenopause, so she adds more cardio. She runs more, takes more spin classes, walks longer distances. The scale barely moves. She feels exhausted. She concludes that exercise "is not working."
The missing piece is almost always resistance training.
As discussed earlier, menopause metabolism changes are driven in large part by the loss of lean muscle mass. Cardio burns calories during the session. Strength training builds the metabolic engine that burns calories all day — even at rest. Every kilogram of muscle tissue burns approximately 13 calories per day at rest, compared to roughly 4.5 calories for a kilogram of fat. Building and preserving muscle is the most powerful long-term lever available for menopause weight management.
Beyond metabolism, resistance training delivers benefits that are uniquely critical during menopause. It improves bone density — directly counteracting the accelerated bone loss that follows estrogen decline. It preferentially reduces visceral fat, even when total body weight changes only modestly. It improves insulin sensitivity, reducing the insulin resistance menopause commonly drives. And it builds the functional strength that makes daily life easier and injury less likely.
A 2020 meta-analysis published in Menopause: The Journal of The North American Menopause Society found that resistance training in postmenopausal women produced significant reductions in visceral fat, waist circumference, and fasting insulin — independent of changes in total body weight.
The practical recommendation: at least 2 strength training sessions per week, targeting all major muscle groups. This does not require a gym membership or heavy equipment. A structured bodyweight routine — squats, lunges, push-ups, rows with resistance bands — performed consistently produces measurable results within 8–12 weeks.
A simple starting structure for beginners:
- Session 1 (Monday): Squats, push-ups, resistance band rows, glute bridges — 3 sets of 10–12 repetitions each
- Session 2 (Thursday): Lunges, overhead press, deadlifts with light dumbbells, plank holds — 3 sets of 10–12 repetitions each
Progress by increasing resistance or repetitions every 2–3 weeks.
The role of aerobic exercise and daily movement
Strength training is the priority — but aerobic exercise still plays an important supporting role, particularly for cardiovascular health and mood regulation.
Current guidelines from NAMS and the British Menopause Society recommend at least 150 minutes of moderate-intensity aerobic activity per week. This breaks down to 30 minutes, 5 days per week — or 50 minutes, 3 days per week. Alternatively, 75 minutes of vigorous-intensity activity per week achieves equivalent benefits.
Moderate-intensity means you can hold a conversation but feel your breathing increase. Brisk walking, cycling on flat terrain, swimming laps, and dancing all qualify. Vigorous intensity includes jogging, uphill cycling, and aerobics classes.
Combining aerobic and resistance training yields the best outcomes. A 2019 study in Obesity Reviews found that midlife women who combined both forms of exercise achieved 5–10% greater total fat loss and significantly better waist circumference reductions compared to those doing either form alone.
Beyond structured exercise, NEAT — non-exercise activity thermogenesis — deserves serious attention. NEAT refers to all the calories burned through movement that is not formal exercise: walking to a meeting, standing at a desk, taking the stairs, gardening. Research suggests NEAT can account for 200–400 additional calories burned per day in active individuals compared to sedentary ones — a difference that compounds significantly over weeks and months.
Practical NEAT strategies:
- Take a 10-minute walk after each main meal
- Stand for at least 30 minutes during every 2 hours of sitting
- Park farther away or get off public transport one stop early
- Take phone calls standing or walking
These small behaviors are genuinely meaningful for menopause weight management, and they are far more sustainable than adding extra gym sessions to an already exhausting schedule.
Practical exercise tips for women with joint pain or fatigue
Joint pain, fatigue, and low motivation are common barriers to exercise during the menopausal transition. Acknowledging this honestly — rather than simply urging women to push through — is important.
Several women I have worked with in my practice arrived unable to walk for more than 15 minutes without knee or hip discomfort. Starting with low-impact alternatives was not "giving up" — it was the smart clinical approach.
Effective low-impact options for menopause weight management include:
- Swimming and water aerobics: Buoyancy reduces joint load while resistance builds muscle
- Cycling: Low impact on knees and hips; can be done indoors on a stationary bike
- Yoga and Pilates: Build core strength, improve flexibility, and reduce cortisol — addressing both physical and hormonal components
- Walking: Underrated and deeply evidence-based; a consistent 30-minute daily walk reduces visceral fat, improves insulin sensitivity, and supports sleep quality
The most important principle at the beginning is consistency over intensity. A 20-minute walk performed 5 days per week produces better 6-month outcomes than an intense 90-minute session performed once. The body adapts to what it experiences regularly — not to what it experiences occasionally.
One client I worked with — a 52-year-old teacher with significant knee pain — began with two 15-minute walks per day and one chair-based strength session per week. Within 6 months, she had lost 6.5 kg, reduced her waist circumference by 8 cm, and progressed to full standing resistance training twice weekly. The starting point was humble. The results were not.
Sleep, stress, and the behavioral side of menopause weight management
Most weight management programs focus almost entirely on food and exercise. For menopausal women, that is not enough. Sleep quality, stress levels, and behavioral patterns are not secondary factors — they are primary drivers of whether nutrition and exercise efforts actually produce results.

How to improve sleep quality during menopause
The target is clear and evidence-based: 7 or more hours of sleep per night. Research consistently shows that women sleeping fewer than 6 hours per night have significantly higher rates of obesity, insulin resistance, and cardiovascular disease than those sleeping 7–9 hours — independent of diet and exercise habits.
For menopausal women, achieving this is complicated by vasomotor symptoms — the hot flashes and night sweats that fragment sleep even when the woman does not fully wake. Addressing these symptoms medically, when appropriate, is a legitimate part of menopause weight management.
Practical sleep strategies that have strong evidence:
- Consistent sleep and wake times, even on weekends — this anchors the circadian rhythm and reduces cortisol variability
- No screens for 60 minutes before bed — blue light suppresses melatonin production and delays sleep onset
- Bedroom temperature between 16–19°C (60–67°F) — cooler temperatures reduce hot flash frequency and improve sleep architecture
- Limit caffeine after 1:00 pm — caffeine has a half-life of approximately 5–7 hours; an afternoon coffee can still be disrupting sleep at midnight
- Avoid alcohol within 3 hours of bedtime — alcohol may induce drowsiness initially but fragments the second half of the sleep cycle
For women experiencing severe vasomotor symptoms that significantly disrupt sleep, discussing medical options — including hormone therapy or non-hormonal alternatives — with a healthcare provider is appropriate and worthwhile.
Managing cortisol and stress to reduce belly fat
Cortisol and menopause weight are connected through a direct biological pathway. Cortisol signals the liver to release glucose, promotes fat storage in the abdomen, and suppresses the satiety hormones that normally regulate appetite. Chronic stress means chronically elevated cortisol — and chronically elevated cortisol means persistent abdominal fat accumulation, regardless of diet quality.
The life stage of menopause often coincides with peak stress exposure: aging parents requiring care, children leaving home or returning, career transitions, relationship changes. These are real stressors, not character weaknesses — and managing them effectively is a clinical priority.
3 evidence-based cortisol management strategies:
1. 20-minute daily walks in natural environments. A 2019 study in Frontiers in Psychology found that just 20 minutes of walking in a natural setting reduced salivary cortisol levels by an average of 21%. This is one of the most accessible and consistently effective stress-reduction tools available.
2. Diaphragmatic breathing (box breathing). Inhale for 4 counts, hold for 4, exhale for 4, hold for 4. Practiced for 5 minutes, this activates the parasympathetic nervous system and measurably reduces cortisol within a single session. It requires no equipment and no scheduled time.
3. Alcohol reduction. Alcohol is frequently used as a stress management tool — and it creates a biochemical trap. It suppresses cortisol acutely, then triggers a cortisol rebound hours later, worsening both sleep fragmentation and abdominal fat storage the following day.
At MenoVitality, we consider stress management as fundamental to our approach as nutrition or exercise — because the evidence is clear that it is.
Behavior change strategies that actually stick
Knowing what to do is not the same as doing it consistently. This gap between knowledge and action is where most weight management programs fail menopausal women — by providing information without addressing the behavioral infrastructure needed to act on it.
3 behavioral strategies with the strongest evidence for menopausal women:
1. Self-monitoring. Keeping a simple food and activity log — even for just 3 days per week — is one of the most consistently effective weight management tools in the literature. A 2019 study in Obesity found that participants who logged their food for 15 minutes or more per day lost twice as much weight as those who logged minimally. The mechanism is awareness: most people significantly underestimate their caloric intake without tracking.
2. Specific goal framing. Vague goals ("I want to lose weight") produce vague results. Evidence-based weight management programs use a target of 5–10% of starting body weight as the primary goal — specific enough to measure, meaningful enough to produce significant health improvements. For a woman weighing 80 kg, that means a target loss of 4–8 kg. This range is achievable in 3–6 months with consistent dietary and exercise changes.
3. Building a support structure. Social support is an independent predictor of weight management success. This means telling one or two people about your goals, finding an accountability partner, or engaging with a community of women in similar circumstances. At MenoVitality, our community platform exists precisely because isolation is one of the most consistent barriers to sustained behavior change in midlife women.
One final behavioral principle: self-compassion over willpower. Clinical programs that frame setbacks as failures and rely on rigid rule-following produce worse long-term outcomes than those that normalize imperfection, build flexible habits, and treat the participant as a capable adult navigating a genuinely difficult biological transition.
A missed workout is not a reason to abandon the plan. An unplanned meal is not a reason to restart from zero on Monday. Consistency over weeks and months matters far more than perfection over any single day.
Medical options for menopause weight management
Lifestyle changes are the foundation of menopause weight management. But for many women, they are not sufficient on their own — particularly when hormonal disruption is severe, when weight gain has been significant, or when metabolic conditions like insulin resistance are already present. Understanding the medical options available is not a sign of failure. It is good clinical practice.

Does HRT actually help with menopause weight gain?
Hormone Replacement Therapy is one of the most misunderstood topics in women's health — and the confusion has real consequences for the women trying to make informed decisions about their bodies.
Here is what the evidence actually says.
HRT does not cause weight gain. This is one of the most persistent myths in menopause medicine, likely stemming from early formulations of synthetic progestins and from misinterpretation of the 2002 Women's Health Initiative trial. More than two decades of subsequent research have clarified the picture considerably.
What hormone therapy and weight loss menopause research consistently shows is more nuanced: HRT does not produce meaningful total weight loss, but it does meaningfully change where fat is stored. Specifically, estrogen therapy reduces visceral fat accumulation, improves insulin sensitivity, and lowers the risk of progression to type 2 diabetes in appropriately selected postmenopausal women.
A 2023 clinical review from Mayo Clinic summarized the evidence clearly: menopausal hormone therapy shifts fat distribution away from the abdomen, improves metabolic markers, and supports a healthier body composition — even when the number on the scale changes only modestly.
The North American Menopause Society and the British Menopause Society both maintain that HRT is appropriate for symptom relief and bone protection in younger postmenopausal women, and that its metabolic benefits are a meaningful secondary advantage — not the primary indication. HRT should not be prescribed purely as a weight-loss drug.
What this means practically: if you are experiencing significant vasomotor symptoms — hot flashes, night sweats, sleep disruption — that are undermining your ability to sleep, exercise, and manage stress, HRT may address multiple drivers of menopause weight gain simultaneously. The conversation with your doctor should cover your individual symptom burden, personal health history, and risk profile.
One patient I worked with — a 49-year-old accountant experiencing 12–15 hot flashes per day — had been unable to sleep more than 4 hours per night for 8 months. No dietary change or exercise program was going to work effectively in that context. After starting HRT under her gynecologist's supervision, her sleep normalized within 6 weeks. Her weight management efforts then began producing results for the first time in over a year.
GLP-1 medications and what they mean for menopausal women
GLP-1 receptor agonists — including semaglutide (Ozempic, Wegovy) and the dual agonist tirzepatide (Mounjaro, Zepbound) — represent the most significant development in obesity pharmacology in decades. Their relevance to menopause weight management is substantial and growing.

Clinical trial data are striking. The STEP 1 trial of semaglutide found average weight loss of 14.9% of starting body weight over 68 weeks in adults with obesity. The SURMOUNT-1 trial of tirzepatide produced average losses of 20.9% over 72 weeks. Subgroup analyses of postmenopausal women show comparable results — with the additional finding that GLP-1 medications preferentially reduce visceral fat, directly targeting the most metabolically harmful component of menopause belly fat.
Early research suggests that combining GLP-1 medications with hormone therapy may produce modestly greater reductions in visceral fat and waist circumference than either treatment alone — though this data is still preliminary and larger dedicated trials are needed.
These medications work by mimicking the GLP-1 hormone naturally produced in the gut after eating. They slow gastric emptying, reduce appetite signals, improve insulin secretion, and lower post-meal blood sugar. For menopausal women dealing simultaneously with insulin resistance, increased appetite from disrupted leptin and ghrelin signaling, and hormonally driven fat storage, this mechanism addresses multiple problems at once.
However, specific concerns apply to this population and deserve honest discussion:
Muscle loss risk. GLP-1 medications reduce total body weight — but a portion of that loss can be lean muscle mass rather than fat. In menopausal women already experiencing sarcopenia, this is a meaningful concern. Mitigating this requires adequate protein intake (minimum 1.2–1.6 g per kilogram of body weight per day) and consistent resistance training throughout treatment.
Bone density. Rapid weight loss of any kind can reduce bone density. This risk is amplified in postmenopausal women, for whom osteoporosis is already a significant concern. Monitoring and supplementation with calcium and vitamin D are clinically appropriate during GLP-1 treatment.
Weight regain after stopping. Clinical data show that most of the weight lost on GLP-1 medications returns within 12 months of discontinuation without ongoing lifestyle support. These medications manage a chronic condition — they do not cure it. The behavioral and nutritional foundations discussed throughout this article remain essential whether or not medication is used.
Cost and access. GLP-1 medications remain expensive in many healthcare systems, with monthly costs ranging from $800–$1,300 USD without insurance coverage. Access is not equitable, and this is a genuine limitation.
At MenoVitality, our position on GLP-1 medications reflects the emerging clinical consensus: they are a powerful tool in the toolbox — not a replacement for lifestyle change, and not appropriate for everyone, but genuinely transformative for women who meet clinical criteria and have access to appropriate medical supervision.
Supplements for menopause weight management — what the evidence says
The supplement market targeting menopausal women is enormous — and largely unregulated. Claims range from plausible to entirely unsupported. Cutting through the noise requires understanding what the evidence actually shows.
What has meaningful supporting evidence:
Magnesium plays a role in over 300 enzymatic reactions including glucose metabolism and insulin signaling. Many menopausal women are deficient. Supplementation at 300–400 mg per day has shown modest improvements in insulin sensitivity and sleep quality in clinical trials — both relevant to menopause weight management. Magnesium glycinate and magnesium citrate are the most bioavailable forms.
Omega-3 fatty acids (EPA and DHA from fish oil) reduce chronic low-grade inflammation — one of the underlying drivers of visceral fat accumulation and insulin resistance menopause promotes. A 2021 meta-analysis found that omega-3 supplementation at 2–3 g per day produced modest but significant reductions in waist circumference and triglycerides in postmenopausal women.
Vitamin D deficiency is extremely common in midlife women and is independently associated with obesity, metabolic syndrome, and cardiovascular disease. Supplementation to achieve serum levels of 50–80 nmol/L is broadly recommended and supports both metabolic health and bone density.
Probiotics targeting specific strains — particularly Lactobacillus and Bifidobacterium species — show emerging evidence for supporting gut microbiome diversity and improving post-menopause weight loss outcomes, though research is still developing and strain-specificity matters significantly.
What to approach with caution:
Proprietary "menopause metabolism blends" with undisclosed dosages, products making unverified fat-burning claims, and supplements containing stimulants like synephrine or high-dose caffeine all warrant skepticism. The FTC and FDA have taken enforcement action against numerous menopause supplement brands for unsubstantiated claims.
The honest summary: supplements can support a well-constructed menopause weight management strategy — but they cannot substitute for one. The foundation remains nutrition, exercise, sleep, and stress management. Supplements fill genuine gaps within that foundation.
MenoVitality — your partner in menopause weight management
Understanding the science of menopause weight management is the first step. Having the right support to act on it is the next.
MenoVitality was built specifically for women navigating the hormonal, metabolic, and emotional complexity of the menopausal transition. Our approach is grounded in the same evidence presented throughout this article — clinical research, professional guidelines, and real-world experience with the challenges midlife women actually face.

Our product range is formulated with transparency and clinical intent: clearly disclosed ingredients, evidence-informed dosages, and no proprietary blends designed to obscure what you are actually taking. We believe every woman deserves to understand exactly what she is putting in her body and why.
Beyond products, MenoVitality offers an educational community platform where women share experiences, ask questions, and support each other through one of life's most significant transitions. Because as the behavioral evidence makes clear — connection and community are not optional extras in menopause support. They are core to sustainable outcomes.
Explore MenoVitality's menopause support range and find the tools that fit your stage →
Frequently asked questions about menopause weight management
How much weight do most women gain during menopause?
Research cited by the British Menopause Society indicates an average gain of approximately 1.5 kg per year during perimenopause, with total gains of 5–10 kg by the time full menopause is reached. However, this varies significantly between individuals based on genetics, starting weight, activity levels, and dietary patterns. Weight gain during this phase is common — but it is not inevitable with the right approach in place.

Can I actually lose weight during menopause, or is it impossible?
Yes — weight loss during menopause is genuinely achievable, but it requires a strategy matched to the hormonal environment. The women in my practice who achieve the best outcomes combine increased protein intake, consistent resistance training, sleep prioritization, and where appropriate, medical support. Realistic expectations matter: a loss of 5–10% of starting body weight over 3–6 months represents a meaningful, evidence-based target that produces significant improvements in metabolic health markers.
Is belly fat during menopause actually dangerous?
Yes — and this point cannot be overstated. Visceral fat menopause drives is not simply a cosmetic concern. Visceral fat is metabolically active tissue that promotes chronic inflammation, raises LDL cholesterol, impairs insulin function, and significantly elevates the risk of cardiovascular disease, type 2 diabetes, and certain cancers. Managing menopause belly fat is a direct investment in long-term health — not vanity.
Does hormone replacement therapy cause weight gain?
No — this is one of the most persistent myths in menopause medicine. Current evidence consistently shows that HRT does not cause weight gain and may actually improve body fat distribution by reducing visceral fat accumulation. Some women report initial water retention in the first 4–6 weeks of HRT, which typically resolves. The net effect on body composition is neutral to modestly positive for most women. Individual responses vary, and medical consultation is essential.
What is the single most important lifestyle change for menopause weight management?
If forced to prioritize one change, the evidence points most strongly to adding resistance training twice per week. Strength training addresses the root metabolic cause of midlife weight gain — muscle loss and declining resting metabolic rate — in a way that cardio alone cannot. Pair it with a protein target of 1.2 g per kilogram of body weight per day, and you have addressed the two most powerful controllable levers available for menopause weight management.

Sources
- Mayo Clinic — "The reality of menopause weight gain": https://www.mayoclinic.org/healthy-lifestyle/womens-health/in-depth/menopause-weight-gain/art-20046058
- ZOE — "Menopause weight gain and why you should stop dieting": https://zoe.com/learn/menopause-weight-gain
- My Menopause Centre — "Menopause Weight Gain: What's Really Happening": https://www.mymenopausecentre.com/blog/menopause-weight-gain-whats-really-happening-and-what-to-do-about-it/
- North American Menopause Society — Dietary strategies for weight loss practice pearl: https://www.menopause.org/docs/default-source/professional/practice-pearl-dietary-strategies-for-weight-loss.pdf
- PubMed / NIH — Obesity and weight management at menopause: https://pubmed.ncbi.nlm.nih.gov/22978257/
- British Menopause Society — Menopause, nutrition and weight gain: https://thebms.org.uk/wp-content/uploads/2023/06/19-BMS-TfC-Menopause-Nutrition-and-Weight-Gain-JUNE2023-A.pdf
- Healthline — GLP-1 medications for menopause weight gain: https://www.healthline.com/health/menopause/can-you-use-glp-1-medications-for-menopause-weight-gain
- Harvard T.H. Chan School of Public Health — The Nutrition Source: https://www.hsph.harvard.edu/nutritionsource/
- Cleveland Clinic — Menopause and weight gain: https://health.clevelandclinic.org/what-can-i-do-to-avoid-weight-gain-at-menopause
Dr. Laura Hendricks, RDN, MS, NCMP is a Registered Dietitian Nutritionist and Certified Menopause Practitioner with over 12 years of clinical experience specializing in women's midlife health. She holds a Master of Science in Clinical Nutrition and has worked with hundreds of perimenopausal and postmenopausal women in her private practice. Dr. Hendricks has contributed to peer-reviewed women's health publications, consults regularly with gynecologists and endocrinologists, and runs a weekly educational workshop called "Midlife and Thriving" for women over 45. Her work centers on translating complex hormonal science into practical, compassionate, evidence-based guidance that real women can act on.
Read more articles by Dr. Laura Hendricks →
Accuracy and fact-checked disclaimer: This article was written and reviewed by Dr. Laura Hendricks, RDN, MS, NCMP, a credentialed nutrition and menopause specialist. All content is based on peer-reviewed research, clinical guidelines from recognized medical organizations including NAMS and the British Menopause Society, and direct clinical experience. This content is intended for educational and informational purposes only and does not constitute medical advice. Individual health needs vary — please consult your healthcare provider before making changes to your diet, exercise routine, or medication regimen. This article was last reviewed and updated in May 2026.